
Case 10 - Got shafted…
Author: Gokul Sagar Bailur Reviewer: Nick Mani/Nish Cherian
A 70-year old female presents with a fall and sustains a right proximal Femoral shaft fracture (no pain in the leg before the fall). She has been given IV Paracetamol and Morphine but continues to be in pain and discomfort along associated with quadricep muscle spasm. The relatives and nurses are requesting more analgesia. The Trauma & Orthopaedic specialist is asking for application of skin traction/Thomas splint before transfer to the ward.
You elect to perform an ultrasound-guided nerve block as part of a multi-modal pain management strategy.
Clip 1- Left of the screen lateral (Right-Medial, Top -Surface)

Image 1- Sono-Anatomy of the Performed Block
-
Ultrasound-guided Right Femoral Nerve Block
-
Performed within 6hrs of the same/similar block
Infection over/around the injection site
Open wound at the site of injection/Intravenous drug user with acive injection site
Vascular surgery such as a bypass
NB anticoagulation/potent antiplatellets are ONLY a relative contraindications. It is an absolute contraindication when the procedure is performed anatomically/blind (https://www.ra-uk.org/images/Documents/RAPAC_for_consultation.pdf)
-
A - Fascia Iliaca
B - Femoral Nerve
C - Femoral Artery
D - Fascia Lata -
Levobupivacaine 0.5% (or equivalent), approximately 10-20ml (max 2mg/kg) in adults >50kg
Alternatively, ropivacaine 0.75%, approx 15-20ml (max 3mg/kg)
A low volume and high concentration is preferable for targeted nerve blocks, compared to plane blocks which require larger volume (and diluted LA) to spread along the fascial plane.
-
As per AABGI guideline.
Know where your 20% lipid emulsion is kept!
https://anaesthetists.org/Home/Resources-publications/Guidelines/Management-of-severe-local-anaesthetic-toxicity
Sono-Anatomy & Technique
General Approach to Scanning for Femoral Nerve
Place the linear transducer along the inguinal crease as shown below. Try to visualise the Femoral Vein which is the medial most vessel, Femoral Artery which is lateral to the Vein and the Femoral Nerve that looks like a triangular hyper-echoic bunch of Grapes.

Image 2 - Surface Anatomy of Different Hip/Pelvis Blocks
FICB (II)- Fascia Iliaca Compartent Blcok Infra-Inguinal, FICB (SI)- Fascia iliaca Compartment Block Supra-Inguinal, FN- Femoral Nerve Block, PENG- Peri-Capsular Nerve Group Block

Image 3 - Femoral Nerve Block (FNB) (Anterior Pelvic Skeletal View)
ASIS- Anterior Superior Iliac Spine, LFCN- Lateral Femoral Cutaneous Nerve, FN- Femoral Nerve, ON- Obturator Nerve

Image 4- Ergonomicology/Safety
Patient, Performer, Assistant, Equipment, Monitoring, Check-list/Stop Before You Block
Note- the ultrasound machine is at the opposite side of the bed for this bloc
Clip 2 - Sono-Anatomy of the Performed Block with Annotations (FA- Femoral Artery)
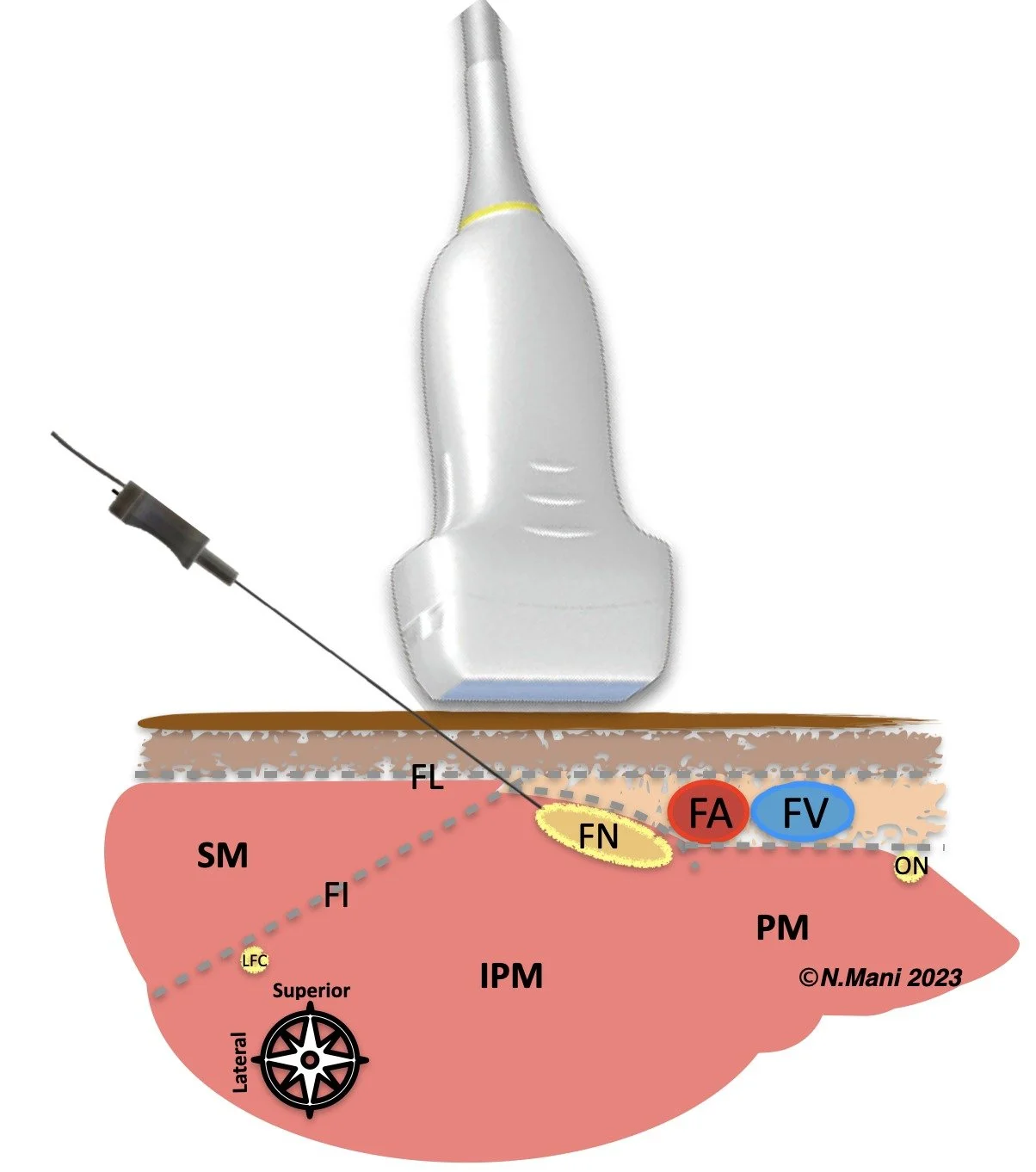
Image 5- Cartoon demonstration of Femoral Nerve Block (FNB) In-Plane
SM- Sartorius Muscle, IPM- Iliopsoas Muscle, PM- Pectinous Muscle, FL- Fascia Lata, FI- Fascia Iliaca
FN- Femoral Nerve, FA- Femoral Artery, FV- Femoral Vein, ON- Obturator Nerve, LFC- Lateral Femoral Cutaneous Nerve
Case RESOLUTION
Patient had an effective analgesia and resolution of the quadricep spasm with the ultrasound guided femoral nerve block, and did not require any further analgesics.
Skin traction/Thomas splint was applied, and patient was admitted to the orthopaedic ward overnight until she had surgery the next day.