
Case 29 - When Push Comes to Shove...
Author: Dr Gokul Sagar Bailur Reviewer/Editor: Dr Julia Burkert-Milone/Dr Nick Mani
A fit and well, middle aged lady is seen in the Emergency Department complaining of 3 months of ongoing and worsening cough, breathlessness , fatigue with significant reduction of exercise tolerance. For the last 24hrs, she has exprienced left sided ongoing blurred vision.
On examination, vital signs are stable, airway to exposure intact, but there is reduce visual acuity and fields in the left eye. ECG — sinus tachycardia with global T-wave Inversion.
You decide to perform bedside focused echo as an extension of standard clinical assessment : -
Clip collection - Bedside Focused Echo (click right/left arrows to cycle between clips)
Clips 1: PLAX. Clip 2- PSAX. Clip 3-6: Apical 4 Chambers +/- zoom / Colour Flow Doppler. Clip 7: Subxhiphoid 4-Chamber. Clip 8: IVC
-
Pericardium - Trace of pericardial effusion posterior to the infero-lateral wall.
LV - severely impaired systolic function and dilated.
RV - longitudinal & radial function is impaired.Atria - LA and RA dilated.
IVC - Dilated and <50% collapsible suggesting raised RA pressure. -
Hyperechoic circular structure is seen at the LV Apex.
Differential diagnosis for this could be a mass or a thrombus. -
Eyeballing estimation of LV function -
LV Ejection Fraction is a useful tool to assess systolic function of the LV. When estimated by an advanced practitioner it has been found to have good correlation with calculated EF by Simpsons method.
Fractional Shortening (FS) -
Change in LV internal diameter (LVID) from end-diastole (LVIDd) and end-systole (LVIDs) - It uses the Teicholz formula to estimate LV volumes and hence ejection fraction.
FS (%) = (LVIDd - LVIDs)/LVIDd x 100
FS >25% corresponds to EF >55%
FS <15% corresponds to EF <30%
Limitation - Linear measurements do not take into account Regional Wall Motion Abnormalities & requires regular sinus rhythm (Afib and LBBB leads to error).
Fractional Area Change (FAC) -
Measures ejection fraction by comparing the area of the left ventricle in systole and at diastole. This is obtained from the PSAX view at the mid papillary muscle level. The normal range is approximately 35-65%.
FAC <20% corresponds to EF <30%
Limitation - RWMA may over or under estimate the EF.
Simpson’s Biplane Method -
Calculates the EF from the volume of LV in systole and diastole, both in Apical 4 chamber and Apical 2 chamber view. It is the best measure of LV ejection fraction.
Limitation - Challenging and time consuming. Require good quality image and clear visualisation of the endocardial border. A foreshortened view can overestimate the LV EF.
Tip - LV length both in Apical 4 chamber and apical 2 chamber should ideally be the same.
You decide to perform a more advanced bedside echo:
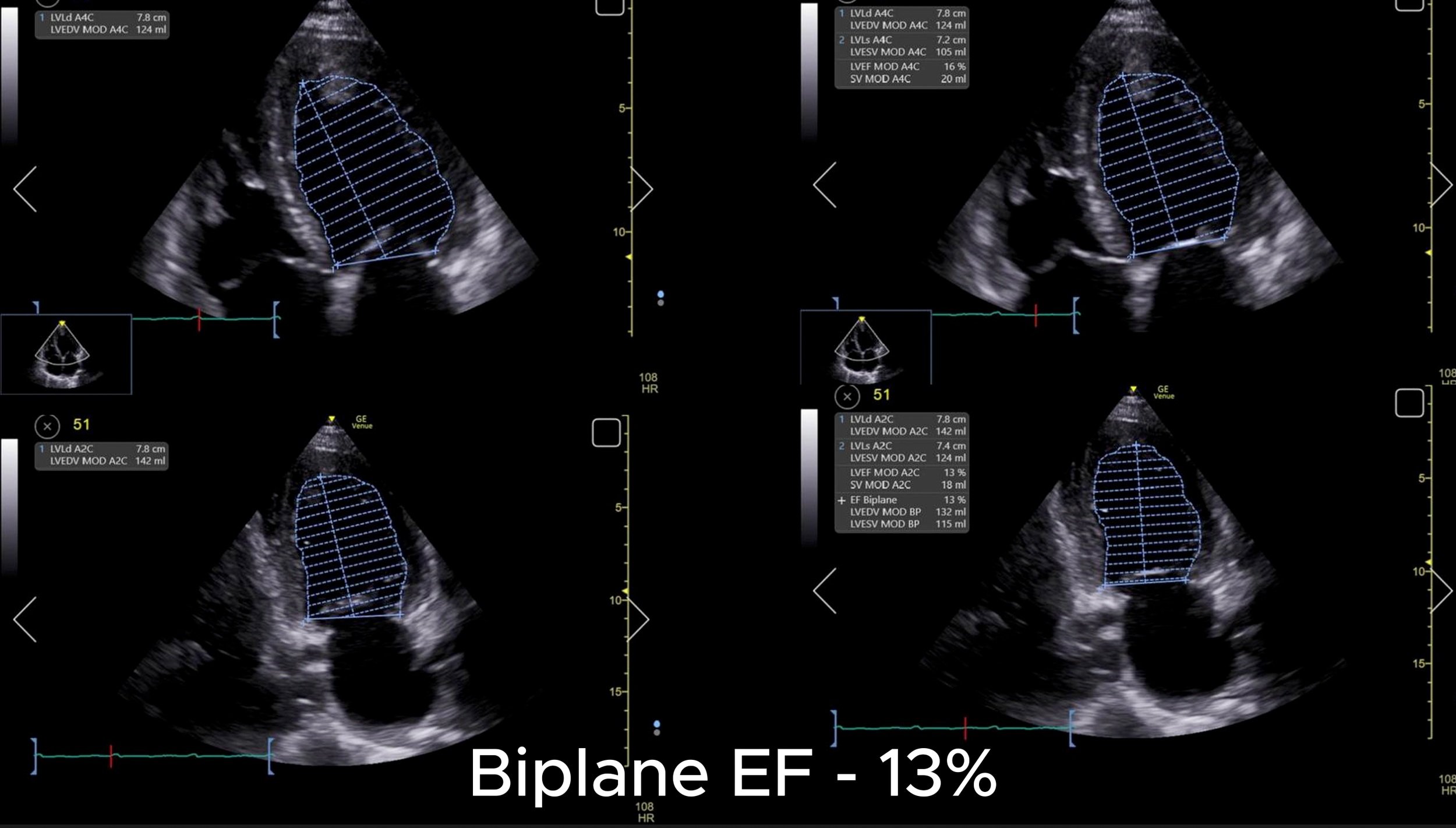


Clip collection - Bedside Focused Echo (click right/left arrows to cycle between clips)
Clip 1: Biplane EF. Clip 2: FS and EF. Clip 3: FAC.
Note- LV ejection fraction does not equate to the Cardiac Output. This depends on multiple factors such as loading/pressures, valvular regurgitation/ stenosis, heart rate/rhythm, amongst other factors.
Whilst in the Emergency Department, the patient suddenly develops left sided ptosis and dysarthria, transferred to resus. Urgent CT head was performed, which showed multiple cerebral ischaemic infarcts likely of cardio-embolic origin.
She was started on anticoagulation after detailed MDT discussion with Stroke, Cardiology and Critical Care Medicine
Case Resolution
Urgent BSE Level 2 echo was performed, which confirmed severe bi-ventricular failure (LV EF of 12%) and an apical thrombus.
Patient was eventually diagnosed to have MRI-positive-myocarditis-induced severe bi-ventricular failure, complicated by an LV thrombus leading to an embolic shower and multiple cerebral infarcts.